Home / All Type of Trauma, Tendon Transfer
Drop Your Number here
Trauma to the face, hand, or upper limb can result from road traffic accidents, industrial injuries, falls, or assaults. These injuries can involve bones, tendons, nerves, vessels, and soft tissues, requiring immediate, specialized surgical care to restore both appearance and function.
Our center offers comprehensive trauma management, from life-saving emergency interventions to microsurgical reconstruction, tailored for every patient.
Facial fractures (mandible, maxilla, zygoma, orbit, nasal bones)
Upper limb fractures (humerus, radius, ulna, hand bones)
Complex hand injuries and crush trauma
Soft tissue lacerations and degloving
Nerve and vessel injuries
Tendon lacerations or rupture
Avulsion injuries and traumatic amputations
Every trauma case is evaluated using imaging (X-rays, CT scans) and clinical examination. We aim to:
Achieve anatomical realignment of bones and joints
Preserve or restore nerve and tendon function
Prevent long-term disability or deformity
Minimize scars and improve cosmetic outcomes
Offer early rehabilitation for faster recovery
Our trauma services are backed by 24x7 surgical availability, microsurgical expertise, and a multidisciplinary team approach including orthopedic, plastic, and rehabilitation specialists.
Restoring Movement When Muscles or Nerves Fail
Tendon transfer is a surgical procedure used to restore movement or strength when a muscle, tendon, or nerve is no longer functional. It involves re-routing a working tendon to take over the job of a paralyzed or injured one.
This technique is often used in cases where nerve injuries (like brachial plexus or radial nerve palsy) have led to permanent muscle weakness or paralysis.
Nerve palsy (radial, median, ulnar, or brachial plexus injuries)
Muscle loss due to trauma or surgery
Birth injuries (Erb’s palsy)
Failed nerve repair or grafting
Spinal cord injuries affecting upper limbs
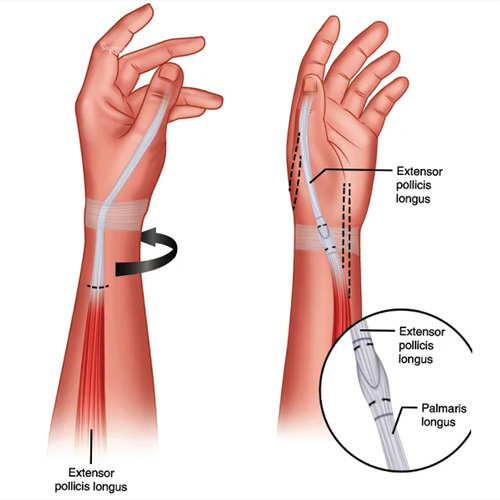
A functioning tendon (from a strong muscle) is detached from its original location and reattached to a tendon of a non-functioning muscle. With post-op therapy, the brain retrains itself to use the new pathway for motion.
Radial nerve palsy: Wrist, finger, and thumb extension restoration
Ulnar nerve palsy: Claw hand correction
Brachial plexus injuries: Elbow flexion or shoulder movement restoration
Spinal injuries: Grasp and release reconstruction
Initial immobilization for 3–4 weeks
Intensive physiotherapy begins thereafter
Brain re-learning phase takes 2–3 months
Full results expected in 4–6 months
Restores functional movement without prosthetics
Avoids repeat nerve surgeries
Can dramatically improve independence and hand use
Reliable outcomes in experienced hands

